A young male, admitted for recent onset seizures.
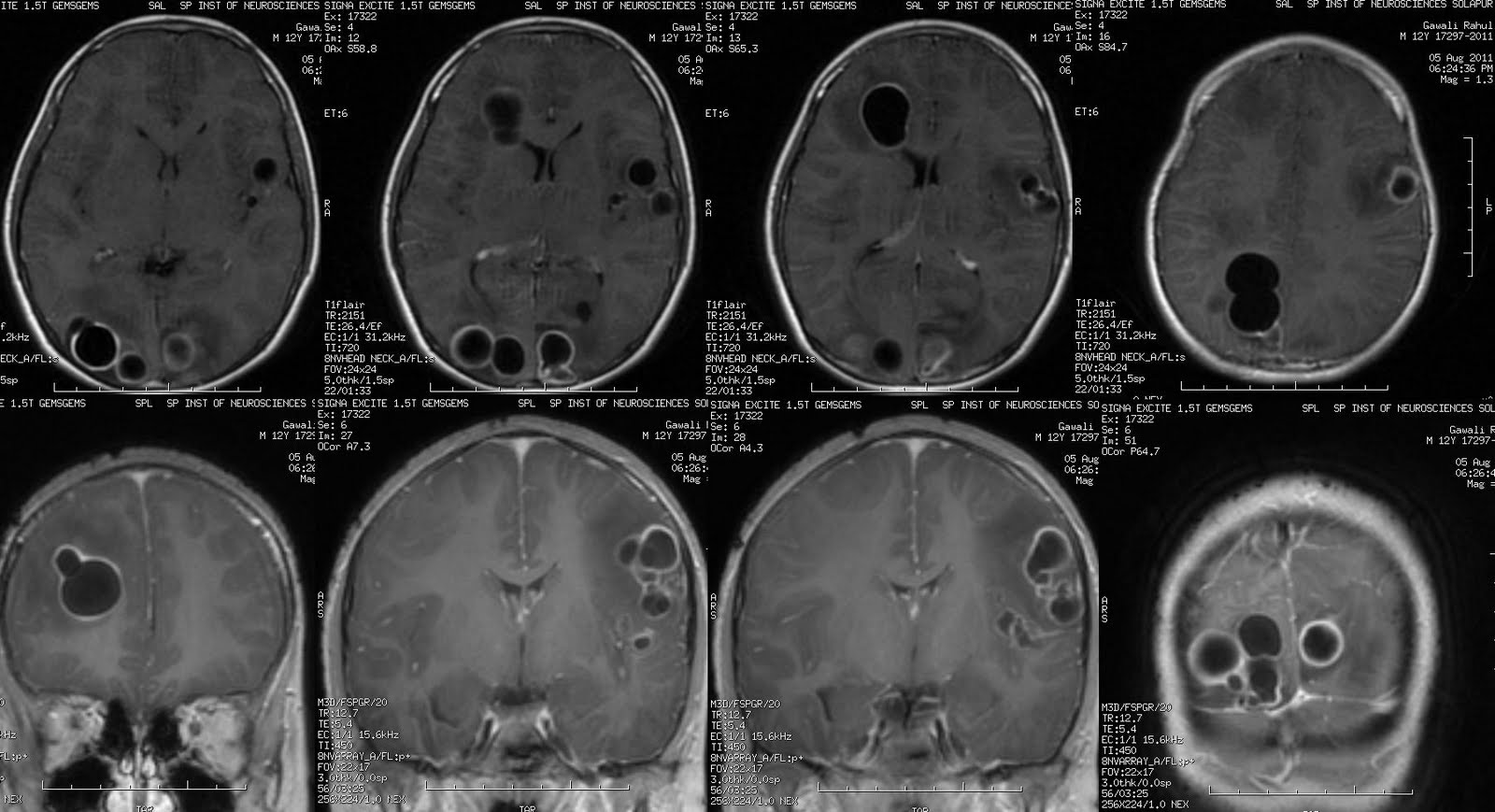
On admission MRI






Description of findings:
A well defined focal lesion in left parietal sub cortical white matter, size ~45x35mm.
Lesion has thin T2 hypointense wall, intensely enhancing on post contrast T1 with a multi locularity, enhancement pattern is peripheral type due to enhancement along its wall, non enhancing necrotic core which is hyper intense T2 and shows restricted diffusion on Diffusion weighted images.
Marked perilesional T2 hyperintense vasogenic odema. Left lateral ventricle is compressed.
No significant mass effect.
Imagingwise Possible DDs: Abscess > Glioma.
Restricted diffusion goes in favor of an Abscess over Glioma.
Histopathology Report : Xanthogranulomatous inflammation, macrophages, granulation tissue with fibroblasts surrounding necrotic core S/o Pyogenic abscess.
Related post :
Abscess MR Spectroscopy