MRI study of hip joints shows:
Avascular necrosis involving bilateral capital femoral epiphysis.

Modified Kerboul method is used for prediction of collapse in femoral head osteonecrosis by volumetric analysis on MRI.
HOW IS IT CALCULATED ?
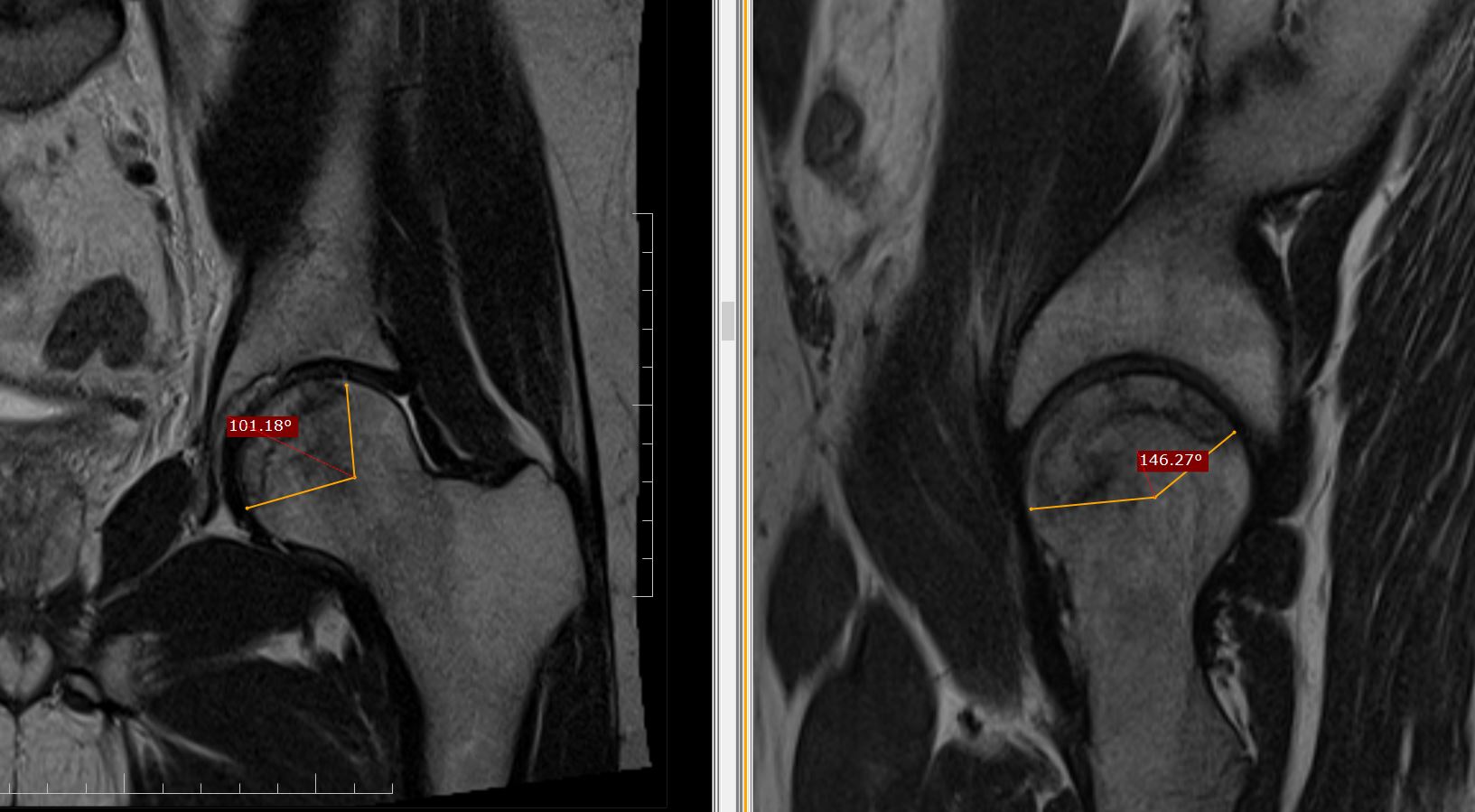
The arc of the femoral surface involved by necrosis measured by angles on midcoronal (A) and midsagittal image (B) and then modified Kerboul angle (A+B) calculated by the sum of the two angles for both the joints.
Right side the angle is (129+169) =298, grade 3 lesion.
Left side the angle is (100+146)
=246, grade 3 lesion.

GRADING
On the basis of combined angle, hips are classified into four categories:
Grade 1 (<200 degrees),
Grade 2 (200 degrees to 249 degrees),
Grade 3 (250 degrees to 299 degrees), and
Grade 4 (>/=300 degrees).
BACKGROUND
The hypothesis is that the combined necrotic angle measurement from magnetic resonance imaging scans predicts the subsequent risk of collapse in hips with femoral head necrosis.
With use of the modified method of Kerboul et al., Angle calculated by sum of the arc of the femoral surface involved by necrosis on a midcoronal as well as a midsagittal magnetic resonance image calculated on MRI, rather than on an anteroposterior and a lateral radiograph is far more accurate than on X-ray.






